


CORTICOSTEROIDS AND ANTIBIOTICS OFTEN AREN’T ENOUGH FOR MARGINAL KERATITIS
WHILE WE, as O.D.s, typically think of meibomian gland dysfunction (MGD), blepharitis and demodex when we hear “lid disease,” we must not forget bacterial, or Staphylococcal (S.), marginal keratitis.
Here, I discuss the etiology, symptoms, clinical signs, diagnosis/management and list the ICD-10 codes for S. marginal keratitis.
ETIOLOGY
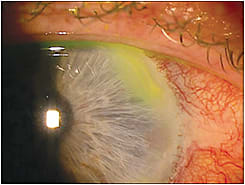
S. marginal keratitis is a sometimes-chronic inflammatory keratitis that occurs in the cornea’s periphery and can cause epithelial breakdown and ulcer development. It is often linked with contact lens contamination from MGD and blepharitis.
Specifically, S. bacteria from the biofilm on the lids or from inside the meibomian glands produces bacterial waste, or byproducts, that enter the tear film and, thus, get spread onto the ocular surface and cornea. These bacterial antigens then trigger an immune hypersensitivity reaction that leads to the production of corneal infiltrates. These infiltrates are usually small and located near the limbus.
S. marginal keratitis can be self-limiting in asymptomatic patients and mild to moderately symptomatic in other patients. The latter patients often require therapy, as the condition can worsen, inducing corneal inflammation and ulceration between 24 to 48 hours of onset.
| Marginal corneal ulcer | H16.04 |
| Unspecified corneal ulcer | H16.00 |
| Other keratitis | H16.8 |
| Unspecified keratitis | H16.9 |
SYMPTOMS
Common symptoms include:
- Corneal pain
- Foreign-body sensation
- Photophobia
- Tearing
CLINICAL SIGNS
The common red flags for S. marginal keratitis:
- Conjunctival hyperemia
- Circular, non-staining stromal infiltrates, usually 1mm to 2mm, separated by a clear zone and located in the cornea’s periphery, usually at the 2, 4, 8 and 10 o’clock position (HSV keratitis, which looks similar to S. marginal keratitis, lacks the clear zone, blepharitis, stromal involvement early on and has a fine area of vascularization bridging and corneal hypoesthesia.)
- Epithelial staining infiltrates/ulceration in more severe and chronic cases
- Intact overlying epithelium (unlike an infectious ulcer, which has epithelial staining when fluorescein is placed on the eye)
- Residual stromal scars or pannus from previous and chronic cases
- Endothelialitis (less common)
- S. blepharitis, which makes the lids present with crusting, scaling, lash and lid debris, lid edema and telangiectasia
DIAGNOSIS/MANAGEMENT
Slit lamp exam shows the clinical signs of S. marginal keratitis.
In terms of treatment, have contact lens wearers discard their lenses and cases and cease lens wear with new lenses until the condition resolves via therapeutic intervention (explained below). Further, reinforce the importance of lens hygiene, discussing the rubbing of lenses with fresh lens solution nightly, replacing lens cases every three months and following the lens-replacement schedule.
Regarding therapeutic intervention, prescribe a combination corticosteroid and antibiotic drop to be used q.i.d. to q.d. for about a week, or until the signs and symptoms resolve. (Sometimes, a stromal scar will remain, which can be asymptomatic and not concerning.)
The antibiotic helps decrease the bacterial load on the lid margin while also adding anti-infective coverage, decreasing inflammation and helping to prevent a secondary infection. A caveat: Do not prescribe topical steroids in patients who have a known history of HSV or who wear contact lenses, as doing so can make the virus proliferate, worsening the keratitis.
In severe and chronic cases of the condition, prescribe topical antibiotic ophthalmic ointments q.d. to b.i.d. short-term, and then q.d. for long-term use.
Finally, as the root cause of S. marginal keratitis is lid margin disease, educate patients on the importance of proper lid hygiene: washing hands prior to use, removing any make-up or lotions around the eyes and using a horizontal motion to gently wipe the base of all the upper lid lashes with the preferred product b.i.d. to q.i.d. for severe cases and q.d. for long-term care. I often see patients who have been treated elsewhere with just a combination topical corticosteroid and an antibiotic.
WATCH FOR IT
While not clinically challenging, we, as O.D.s must be able to diagnose marginal keratitis, as it’s a common issue seen in clinic. Also, it’s important to remember adjunctive lid hygiene treatments to make this sometime-chronic infection a less frequent nuisance. OM
