


WHAT KIND OF TRAUMATIC RETINOPATHY DID THIS PATIENT HAVE?
A 45-YEAR-OLD African-American male presented with a complaint of decreased vision OD for one year. He said someone elbowed him in this eye about a year ago during a basketball game and that he did not seek treatment at that time. The patient denied symptoms of floaters or flashes of light and any systemic history or medication use.
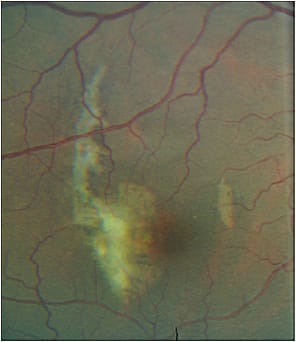
BCVA was 20/40 OD, with no improvement on pinhole, and 20/20 OS. Pupils, ocular motilities and confrontation VF testing were unremarkable OU. IOPs were 12 mmHg OD and OS, and anterior segment was unremarkable OU. Gonioscopy revealed no angle recession OD. A crescent, yellowish lesion with pigmentary hyperplasia was noted temporally to the macula OD with no hemorrhages. No holes, tears or detachment of the peripheral retina OD was found, and OS was normal in these areas. SD-OCT imaging revealed disruption in the retinal pigment epithelium (RPE), choriocapillaris (CC) and inner segment/outer segment (IS/OS) layers, with no evidence of a choroidal neovascular membrane or macular edema OD.
Blunt trauma to the retina can lead to an array of complications, such as traumatic retinal detachment or tear, macular hole or vitreous hemorrhage. (See “What Caused This Detachment?” at http://bit.ly/2rJIjYl .) Yet, these conditions were not observed, so what other traumatic retinopathies may have caused this patient’s symptoms and clinical findings?
Here, I provide an overview of the traumatic retinopathies, their clinical symptoms/signs, diagnosis and management and the answer.
| Choroidal rupture | H31.32 |
| Other injuries of right eye and orbit (Commotio retinae) | S05.8X1A |
| Purtscher’s retinopathy | H34.9 |
TRAUMATIC RETINOPATHIES
Blunt ocular trauma, which may arise from situations, such as sports injuries, fistfights, falls, motor vehicle accidents or projectile injuries (BB or paint ball guns), can result in serious damage to the retina. In fact, more than 60% of the estimated 2.4 million eye injuries per year in the United States result from blunt injury to the eye, reveals Ophthalmology. Retinal complications of blunt trauma span a range of conditions, including choroidal rupture, commotio retinae (Berlin’s edema) or Purtscher’s retinopathy.
- Choroidal rupture. This is a tear in the choroid, Bruch’s membrane and RPE triggered by a blunt injury that exerts stress on Bruch’s membrane, which is less elastic, leading to fracture. Up to 10% of patients with blunt trauma develop a choroidal rupture, reports Archives of Ophthalmology. A higher prevalence exists among male children or those involved in organized sports or games, states the American Journal of Ophthalmology.
- Commotio retinae (Berlin’s edema). This is a self-limiting condition that presents as an area of whitish opacification of the retina, secondary to blunt injury — specifically, RPE and photoreceptor IS/OS disruption and damage, reports Retina. The lesion can appear over the site of the trauma or on the contralateral side of the globe (countercoup), due to shock waves that traverse from the impact site. When it involves the macula, it is called Berlin’s edema. Also, foveal involvement may appear as a cherry-red spot because the cells involved in the whitening are not present in the fovea.
- Purtscher’s retinopathy. Named for Austrian ophthalmologist, Othmar Purtscher, who described it in 1912, this may occur due to severe head or chest compression injuries. Although the exact pathogenesis is not known, the presumed mechanism includes embolic occlusion, usually confined to the blood supply of the peripapillary retina and macular area. Additionally, a second related entity, termed Purtscher-like retinopathy, is associated with multiple systemic conditions, including thrombotic thrombocytopenic purpura, acute pancreatitis, renal failure, autoimmune diseases (systemic lupus erythematosus) and Valsalva maneuver.
CLINICAL SYMPTOMS/SIGNS
The clinical symptoms/signs of these traumatic retinopathies:
- Choroidal rupture. Symptoms may include vision loss, with signs consisting of variable VF defects, such as isolated scotomas, central or centrocecal defects and enlargement of a blind spot or generalized constriction of the VF. Indirect injuries produce ruptures that are distant to the site of the injury — more in the posterior pole temporal to the optic nerve. Direct injury produces ruptures at the site of the trauma or peripheral ruptures. Choroidal rupture is noted as a curvilinear or crescent-shaped yellow line concentric to the optic nerve. With time, these ruptures evolve in to a white streak with pigmented margins due to RPE hyperplasia. Typically, single lesions exist, but about 25% of patients develop multiple lesions, reports the British Journal of Ophthalmology.
More than 60% of ruptures involve the macula, with up to 20% developing a secondary choroidal neovascularization (CNV) because of the disruption of Bruch’s membrane, reports the British Journal of Ophthalmology. CNV may occur with subretinal hemorrhage and serous detachment, obscuring the rupture and leading to severe vision loss. Also, development of a CNV may occur up to four years or more after the trauma, with more than 80% showing during the first year, reports Archives of Ophthalmology. - Commotio retinae (Berlin’s edema). The main symptom here is a transient decrease in VA, which typically resolves within a few weeks, although persistent visual scotomas have also been reported. Signs consist of a pale, white appearance of the affected retina with a retinae lesion peripherally, typically in the temporal or inferotemporal retina. Transient moderate myopia, presumably due to annular ciliochoroidal effusion, may also occur.
- Purtscher’s retinopathy. Symptoms include varying degree of visual impairment accompanied by either central, paracentral or arcuate scotomata VF loss. Signs include cotton-wool spots, intraretinal or flame-shaped hemorrhages typically confined to the peripapillary retina and macular area. Purtscher flecken (multiple patches of superficial retinal whitening) are considered pathognomonic findings, but only occur in about 50% of cases, reports the British Journal of Ophthalmology. Occasionally, the retinal whitening surrounds the fovea or when extensive macular edema is present. Bilateral disease is generally present, although unilateral cases have been described. Also, although the optic nerve may appear normal initially, an afferent pupillary defect may be present, closely followed by optic nerve edema and pallor as persistent sequelae after several months.
DIAGNOSIS/MANAGEMENT
In addition to a detailed patient history of the blunt force injury (anything that hit the eye, what the patient was doing when the eye was injured, etc.), slit lamp and dilated exam with scleral indentation to rule out a retinal tear, you should also use the following to aid in the diagnosis of traumatic retinopathies:
- Amsler grid and VF test. Amsler can detect any central scotoma or metamorphopsia, which indicates the development of CNV in patients who have a choroidal rupture, or macular involvement in commotio retinae. Automated perimetry is useful in quantifying the variable VF defects observed with each clinical entity.
- Retinal photography. This is necessary for documenting changes through time.
- Fundus autofluorescence (FAF). Choroidal rupture can be observed as a hypoFAF line, while RPE hyperplasia that occurs as the rupture heals may appear as hyperFAF. Imaging of commotio retinae demonstrates hypoFAF with increased hyper FAF in areas where the RPE is damaged. In Purtscher’s retinopathy, FAF may exhibit hypoFAF in the areas corresponding to intraretinal hemorrhage and hyper FAF corresponding to the sites where Purtscher’s spots are observed.
- SD-OCT. This imaging shows two patterns of choroidal rupture: one with forward protrusion of the RPE-choriocapillaris layer with a pyramid or dome shape (Type 1) and a posteriorly concave area of disruption of the RPE-CC (Type 2). Other findings through SD-OCT: loss of photoreceptor IS/OS segment, edema and CNV.
Imaging of commotio retinae may show small transient RPE irregularities and hyper-reflectivity of the IS/OS layer and outer retina in mild contusion. Permanent pigmentary alterations, loss of IS/OS junction and outer retinal atrophy may be observed with severe permanent injury. Also, cystoid macular edema may appear.
Purtscher retinopathy imaging reveals hyper-reflectivity in the inner retinal layers corresponding to cotton-wool spots and a variable degree of macular edema in the acute phase and variable degree of outer retinal atrophy and photoreceptor loss in late phase. - B-scan ultrasonography. This should be performed on any patient with blunt ocular trauma to rule out the above-mentioned conditions when media opacity (e.g., from vitreous hemorrhage or severe cataract) is present. Specifically, the technology aids in the assessment of the retina and choroid for detachment, tear or dialysis.
In terms of management, patients who sustain blunt trauma may require a CT or MRI scan, x-rays and an ultrasound to rule out facial and/or orbital fracture or other neurologic damage, such as optic nerve injury. For patients who have metallic intraocular or intraorbital foreign bodies, CT may be ordered because an MRI causes movement of these objects leading to further injury. Additionally, treatment of concurrent anterior segment complications, such as corneal abrasions or iritis, requires topical antibiotics, cycloplegics or a corticosteroid.
Patients who have a choroidal rupture should be followed closely (monthly for the first six-months) for the development of CNV, retinal tear or detachment. Long-term management should include Amsler grid testing for the development of CNV. Therapeutic options, including anti-VEGF injections or a laser are aimed at managing associated CNV.
No treatment is recommended for patients who have commotio retinae, which may take about one to six months to resolve with recovery of vision. Thus, patients should be followed monthly initially, followed by three to six months follow-up as permanent macular damage, including macular pigment epitheliopathy or macular hole formation, may occur. In the majority of the Purtscher’s retinopathy cases, the acute lesions resolve spontaneously within one to three months after onset. Thus, patients should be followed monthly for the first three months. Permanent damage, optic nerve atrophy or persistent scotomata, require long-term follow-up and VF testing. For those who have Purtscher-like retinopathy, treatment of the underlying condition (pancreatitis, etc.) is paramount. All patients subjected to blunt trauma require long-term monitoring for angle recession glaucoma. All patients subjected to blunt trauma require long-term monitoring for angle-recession glaucoma. Last, but not least, these patients should be advised to protect the good eye via full-time protective eyewear (protective frame with polycarbonate lenses), if one eye has been injured.
THE ANSWER
If you diagnosed this patient with a choroidal rupture, you are correct! Specifically, the patient’s decreased vision resulted from a choroidal rupture that involved the macula area OD with no CNV. Retinal photos and SD-OCT were obtained. He was educated on the finding, given a home Amsler grid and advised to return for a three-month follow-up. He continues to be monitored with six-month visits and remains stable. His vision loss is permanent.
Blunt injury to the eye can cause a number of severe retinal conditions, illustrated above, if not treated quickly and appropriately and can lead to sight-threatening complications. Prompt assessment, co-management and eye health safety education are essential. OM
