


FOR ITS ease of use, image quality and ability to inspire patients to take better charge of their ocular and systemic health, optical coherence tomography angiography (OCTA) is a valuable diagnostic device, some optometrists say.
Aaron Lech, O.D., F.A.A.O., a managing partner of ClearVue Eye Care, in Roseville, Calif., has been using OCTA (ZEISS’ Cirrus 5000 angiography) since October 2016. He says his practice already had been employing the machine for OCT since 2009, so when the angiography capabilities came out, upgrading was a “no-brainer.” He says, “It was a piece that blended well with our clinical footprint.”
Gregory Caldwell, O.D., F.A.A.O., an ocular disease consultant in Duncansville, Pa., says he’s been using OCTA (Optovue’s AngioVue) since September. Dr. Caldwell explains the device has been helpful in detecting any disease that has a vascular component. Dr. Caldwell adds, “You’re talking high blood pressure, AMD, diabetes, even some rheumatological conditions.”
The two doctors provide a tour of the benefits of OCTA.
EASE OF USE
The devices are simple to use. As is the case with OCT, the patient sits in front of the machine and places his chin on the chin rest. Then, he’s directed to look at a target inside the instrument. As he looks, the technician hits a button, and the images are acquired. Built-in eye-tracking software keeps the patient’s eyes aligned. Images can be taken — in many cases — in less than a minute.
In Dr. Lech’s practice, the data uploads from the OCTA device to a diagnostic data management system. Then, in an exam room, Dr. Lech can pull up the images on a program, called “FORUM: Retina Workplace,” to review with the patients.
“It’s very dynamic,” he says. “It’s not like a paper or a printed report. You can scroll through the different levels of the retina . . . You can zoom in, you can pick a particular section, you can dial in to a specific set of blood vessels that look abnormal and, if you detect something you’d like to investigate further, such as an irregular blood vessel or piece of tissue, you can ask the tech[nician] to run a targeted set of images on the device.”
In smaller practices, doctors can review the images directly on the device, Dr. Lech says.
The test is easy to build into your workflow, Dr. Caldwell adds. If he thinks OCTA is warranted, he’ll ask a technician to run the test, and he’ll go see a different patient in the next exam room. By the time he comes back a few minutes later, the images are available for review.
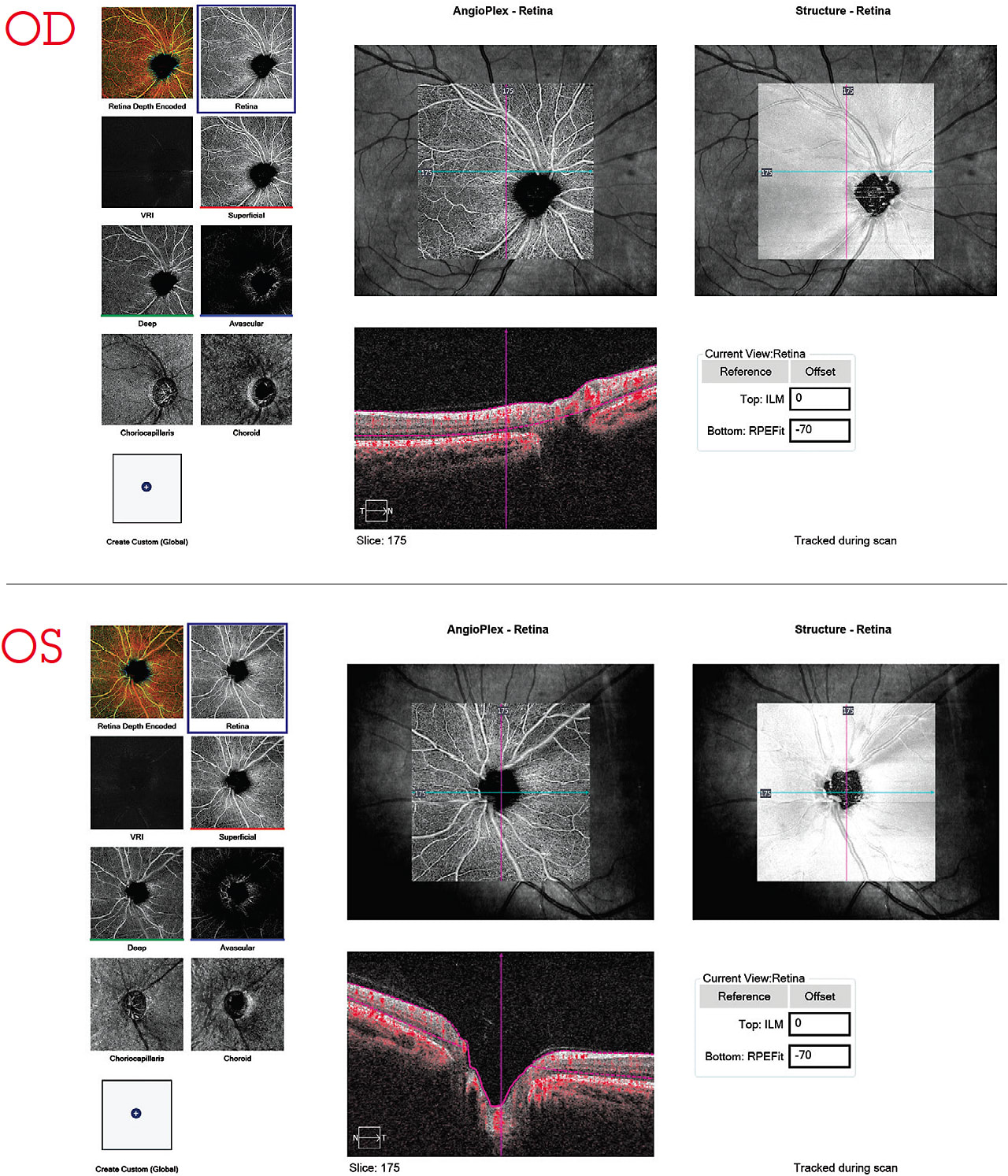
IMAGE QUALITY
The OCTA can reveal disease-related changes in the eye, making a real difference in patients’ lives, the doctors say. Dr. Lech says he saw one woman in her 40s for an annual exam, who previously underwent LASIK and presented with no visual symptoms; her refraction was 20/20 OU. On OCT (Dr. Lech runs baseline OCT and OCTA exams on every patient, only billing insurance based on medical necessity), her optic nerve looked pretty healthy, but with OCTA, he found a section of blood vessels that looked very dark compared with a typical patient. Upon further investigation, he says he realized there were multiple vascular events that had occurred. The patient turned out to have a clotting disorder but was asymptomatic. (See, “The Baseline Exam,” p.20)
“It was the OCTA that picked that up,” he says.
In another instance, Dr. Lech compared optic nerve OCTA scans on a healthy patient’s right and left eye, noticing one was distinctly more dim, but he couldn’t figure out why.
“We actually sent him [the patient] in for a cardiology consult, and he was 90% stenosed on one side of his carotid artery,” he explains. “The patient had a stroke before his scheduled endarterectomy, but because he had started anticoagulant therapy, he fully recovered. “OCTA helped him avoid permanent disability,” Dr. Lech says.
Dr. Caldwell, too, has made some interesting disease finds thanks to OCTA, he says. One man with a history of cataract surgery OD came in complaining of blurry vision in his left eye; he thought it was a cataract because he already had cataract surgery in his other eye. The patient had known non-exudative “dry” AMD. When Dr. Caldwell looked at the back of the eye, he says things looked good, but on OCTA he detected an early membrane. He called a retina specialist and because of the OCTA image, the doctor took the patient right away.
“If we didn’t have the technology, they might have said, ‘Get him in within a week,’” Dr. Caldwell says. “From a systemic disease standpoint, with AMD patients or patients with any type of pigmented epithelial detachments where we’re not sure if a choroidal neovascular membrane is there, we just run the OCTA, and it gives us confidence about what’s going on and how to make an appropriate referral.”
OCTA has been helpful in identifying vascular changes in diabetic patients, Dr. Caldwell adds.
The Baseline Exam
OCTA also can be used for baseline assessment to detect early vascular changes that may indicate the need for closer monitoring, treatment or referral to a specialist. The Optovue system has a built-in report, called “Wellness,” which allows Dr. Caldwell and his colleagues to assess both the retina and the ganglion cell complex for early signs of disease. However, this wellness exam is not medically billable because it is looking for the presence of disease, so patients must pay out of pocket.
“Optovue provides Wellness training tools for the practice staff, so they feel comfortable discussing this option with patients,” Dr. Caldwell says. “Should disease be uncovered, subsequent OCT scans performed on a different day are medically billable.” Both types of scans can help to increase revenue, he notes, thereby offsetting the cost of acquiring the OCTA system.
Dr. Lech’s practice runs baseline OCT scans on every comprehensive exam patient, and OCTA on every diabetic patient, whether they’re controlled or uncontrolled: “That way, we can see definitively if there are any changes in the vasculature.” His office can bill a patient for this test if he acknowledges, via signature, that the scans are not reimbursed or billable to insurance. “The key difference is that the scan run with the baseline exam is the same format used to monitor or diagnose a condition when and if the patient converts to a medical condition,” says Dr. Lech.
INSPIRING PATIENTS
“When these patients see their blood flow, they engage,” Dr. Lech says. “The next time around they’re asking, ‘How did that blood flow look?’ or ‘What does it look like compared to last time?’ They’ll even point to specific areas and ask what that means. The next question they ask is, ‘What can I do about that?’”
Dr. Caldwell says he appreciates being able to demonstrate microaneurysms and capillary dropout in diabetic patients.
“A patient may come in saying, ‘My doctor wants me to get my hemoglobin A1C down to a 7, but I feel pretty good, and I see fine,’” he explains. “Then I show them the changes happening at the microscopic level, which I couldn’t do before. A few months later, people are coming back saying, ‘Hey, I’ve got my hemoglobin a few points lower,’ because they don’t want to lose vision.”
AROUND THE BEND
In the future, look for OCTA tools to measure density and blood flow, Dr. Lech says.
“Being able to grasp blood flow and know what the density of the capillaries looks like in a specific area is going to be very important for progression analysis,” he explains.
A patient’s A1C test or other labs may look good, but if they’re losing density of the capillaries, that is going to create a significant problem downstream, Dr. Lech says.
“Detecting that change in the retinal vasculature is going to be very important,” he explains. “Data scientists are working to develop these tools.” OM