


The choroid plays an important role in the pathogenesis of a number of posterior segment pathologies, including AMD, choroidal tumors, posterior inflammation and diabetic retinopathy.
That said, historically adequate visualization of its structure and function, via techniques such as ultrasound and indocyanine green angiograms has been challenging, due to image resolution limitations. Also, the choroid is not visible with conventional OCT, as the photoreceptor and retinal pigment epithelial (RPE) layers scatter the light signal, resulting in a weak signal from the choroid.
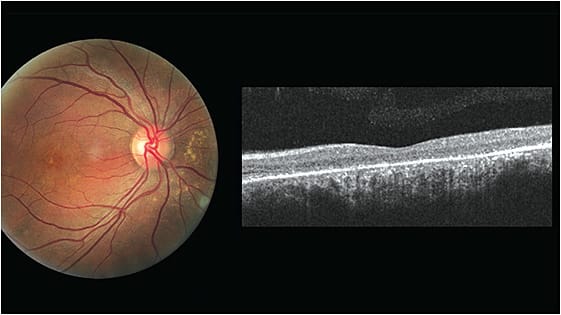
The good news: Enhanced-depth imaging (EDI-OCT) and SD-OCTA have greatly improved our ability to visualize the choroid.
EDI-OCT allows for cross-sectional views that expose variations in the structure and thickness of the choroid; whereas, SD-OCTA provides information about choroidal vasculature, allowing for the detection of choroidal neovascular membrane (CNVM).
As a result, there is improved recognition of CNVM and other choroidal diseases, such choroidal thickening, referred to as the pachychoroid spectrum, which includes conditions, such as central serous chorioretinopathy and polypoidal choroidal vasculopathy.
Here, we discuss the choroid in greater depth and provide an overview of the macular disorders that fall under pachychoroid spectrum and how they differ from AMD.
THE CHOROID
The choroid, the posterior portion of the uveal tract, is a vascularized and pigmented tissue that supplies the outer retina. In fact, it has the highest blood flow per unit weight of any tissue in the body, about 20 times to 30 times greater than that of the retina, reports Survey of Ophthalmology.
The choroid’s innermost layer is the complex five-laminar structure of Bruch’s membrane, and its outermost is the suprachoroid, which is the space between the choroid and sclera. The choroid blood supply comes from branches of the anterior and posterior ciliary arteries, while venous drainage is achieved through the vortex veins. There are three vasculature layers: (1) the inner choriocapillaris (the capillary network); (2) middle Sattler’s layer (consisting of small-medium caliber vessels, especially arteries that originate in the short posterior ciliary arteries) and (3) outer Haller’s layer (consisting of large vessels, especially vortex veins).
The vasculature of the choroid supplies nutrients and oxygen to the outer two thirds of the retinal layers, the avascular fovea and the prelaminar portion of the optic nerve. Thus, compromised choroid blood flow can result in photoreceptor and RPE dysfunction and death.
THE PACHYCHOROID SPECTRUM
The term pachychoroid means an abnormal and permanent increase in choroidal thickness. Choroidal thickness has been reported between 220 μm and 350 μm. A thick choroid is defined as a thickness of 390 μm and higher, reveals Retina.
The pachychoroid spectrum’s multitude of macular disorders share similar features, including increased choroidal thickness, dilation of the choroidal veins (Haller’s Layer) or “pachyvessels,” and retinal pigment epithelium (RPE) abnormalities , according to Retina.
These macular disorders:
- Pachychoroid pigment epitheliopathy (PPE). PPE is believed to be a precursor of central serous choroidopathy, characterized by the presence of RPE abnormalities with absence of preceding or co-existing neurosensory detachment, reports Retina. These RPE abnormalities, such as hyperplasia and drusen-like deposits, may be misdiagnosed as AMD.
Classically, a thickened choroid is denoted on EDI-OCT, which is due to pachyvessels with overlying attenuation of the choriocapillaris and Sattler’s layer, reveals Retina. The pachyvessels run in close proximity to the RPE-Bruch membrane complex, inciting the pigment epithelium changes. - Central serous choroidopathy (CSC). CSC is characterized by a serous neurosensory detachment, often associated with serous pigment epithelial detachments (PEDs). SD-OCTA shows a typical smooth and convex profile of neurosensory detachment, with underlying hypo-reflectivity. EDI-OCT shows a thickened choroid and localized dilated vessels, or pachyvessels, which can also be observed on OCTA. This helps in the differential diagnosis with the subretinal fluid associated with wet AMD.
Although acute CSC is self-limiting, recurrent or chronic CSC (>3 months) disease may result in RPE changes, thickened photoreceptor outer segments, ellipsoid zone disruption and, eventually, outer retinal atrophy and/or neovascularization formation (pachychoroid neovasculopathy), according to Retina. - Pachychoroid neovasculopathy (PNV). PNV is characterized by the presence of Type 1 CNVM associated with a pachychoroid phenotype, such as a chronic CSC, reports Retina. PNV is distinguished from neovascular AMD by several features, including younger age at onset, absence of drusen and a thickened choroid with pachyvessel, as seen on EDI-OCT, reveals Retina. The CNVM network is visualized on SD-OCTA as a tangled network under the pigment epithelial detachments, reports Retina.
Although elderly patients can exhibit clinical features of both PNV and neovascular AMD, the occurrence of Type I CNVM without drusen is uncommon, according to the American Journal of Ophthalmology, further helping you to make a definitive diagnosis of AMD. - Polypoidal choroidal vasculopathy (PCV). PCV is a condition of the inner choroid with polypoidal lesions (polyps) that either have or don’t have branching vascular networks (BVN) below the RPE, but above Bruch’s membrane, suggesting that polypoidal lesions originate from Type 1 CNVM, according to Retina. The clinical findings include recurrent large serosanguinous RPE detachments that may mimic those associated with neovascular AMD.
Unlike AMD, however, PCV patients typically are of Asian and African ancestry, younger, lack drusen and have thicker choroid with pachyvessels. On SD-OCTA, PCV lesions are dome-shaped RPE detachments with double reflective layers (the RPE and highly reflective layer beneath the RPE in the area of the BVN) called the “double-layer sign,” reports Ophthalmology. On EDI-OCT, a darker, circular section in the middle of the polyps are a sign of CNVM, which is observed as a hyper-reflective filamentous vascular network on OCTA, according to the American Journal of Ophthalmology and Retina.
LAYERS OF LEARNING
Our understanding of the choroid has vastly improved in recent years with the advent of advance imaging techniques, such as EDI-OCT and SD-OCTA. These devices have provided new insights on choroidal pathologies, expanded the spectrum of macular diseases, improved early detection, diagnosis and management of a variety of chorioretinal conditions. OM

