


One of the most exciting aspects of practicing optometry is playing a role in the diagnosis of systemic diseases. Included is hematological disorders, which can present with various retinal findings. For example, the recent dilated examination of a 33-year-old black female revealed bilateral retinal hemorrhages and cotton wool spots. Her diagnosis: iron-deficiency anemic retinopathy.
Here, I discuss this, among other retinal findings associated with hematologic disorders, so O.D.s can immediately refer these patients to their primary care physicians for definitive diagnoses and the most appropriate related management and treatment.
ANEMIC RETINOPATHY
Findings: Optometrists note hemorrhages that can present at all levels of the retina and choroid, Roth’s spots, exudates, cotton wool spots, retinal edema or venous tortuosity.
Anemic retinopathy is reversible with correction of the anemia. Retinal vascular occlusions, areas of nonperfusion and neovascularization, or optic nerve pallor may be observed in patients with moderate-to-severe disease.
Hematologic disease: The condition is most likely to occur in patients who have severe (hemoglobin concentration < 6 g/dL, hematocrit value <45) or when thrombocytopenia, a disorder of low platelets, is coexistent.
Background: Anemias occur when the level of healthy red blood cells or hemoglobin (an iron-binding, oxygen-carrying protein within the red blood cells) is too low. This can result from nutritional problems, such as an iron deficiency (most common type), vitamin deficiency (lack of vitamin B12 is known as pernicious anemia) or folate deficiency.
Other causes of anemia are blood loss, inadequate production of red blood cells (aplastic anemia) or increased destruction of red blood cells (hemolytic anemia) that may present lifelong health problems, such as infections that last a long time, and easy bruising or bleeding or serious medical conditions, such kidney failure, arrhythmia or heart failure.
Anemia may also occur due to long-term (chronic) medical conditions, such as cancers (lymphoma), infections (hepatitis) or autoimmune disorders (rheumatoid arthritis or systemic lupus erythematosus).
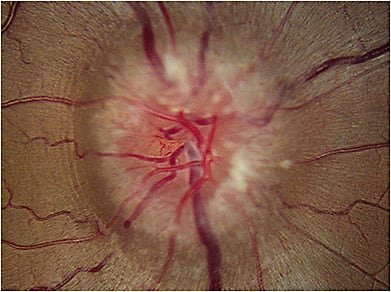
LEUKEMIC RETINOPATHY
Findings: O.D.s see multiple preretinal and intraretinal hemorrhages that are most commonly found in the posterior pole. Other features of this retinopathy include Roth’s spots (possibly representing small areas of retinal leukemic infiltration or platelet fibrin deposits), cotton wool spots, exudates, retinal venous tortuosity, perivascular sheathing, macular edema and vitreous hemorrhage. Peripheral neovascularization or sea fans neovascularization (reminiscent of sickle cell retinopathy) may develop in patients who have chronic leukemia.
Choroidal infiltration can result in a serous, or exudative, retinal detachment, while optic nerve infiltration may result in swelling or pallor, usually a poor prognostic indicator.
Hematologic disease: Found in both the acute and chronic forms of leukemia.
Background: Leukemia is a neoplastic blood disorder characterized by the overproduction of abnormal white blood cells. It can be divided into two types; myelogenous and lymphocytic. Leukemia is further divided into acute myelogenous leukemia, acute lymphocytic leukemia, chronic myelogenous leukemia or chronic lymphocytic leukemia. The reported prevalence of ocular involvement in leukemia is as high as 90%, reports the American Journal of Ophthalmology.
LYMPHOMA RETINOPATHY
Findings: These retinal abnormalities are divided anatomically into vitreoretinal and uveal forms. The vitreoretinal form is a variant of primary central nervous system lymphoma, typically a large B-cell tumor and associated with poor prognosis. The hallmark of the vitreoretinal form is the presence of fine vitreous cells and focal or diffuse subretinal pigment epithelium deposits.
The uveal form’s retinal findings include multifocal, creamy, yellow-white choroidal lesions, chorioretinal folds, obscuration of choroidal vessels, or retinal detachments.
Additionally, retinal phlebitis, cotton wool spots and non-resolving uveitis have been reported.
Hematologic disease(s): The vitreoretinal form is associated with primary central nervous system non-Hodgkin’s lymphoma. The uveal form is associated with systemic non-Hodgkin’s lymphoma.
Background: Lymphoma is a malignant neoplasia of white blood cells of lymphocytic origin. Lymphomas may be derived from B or T lymphocytes, but the lymphomas that affect the eye are primarily of B-cell origin. Lymphomas are divided into two categories: Hodgkin lymphoma, the most common, and non-Hodgkin lymphoma. Orbital involvement is a rare complication of Hodgkin’s disease, whereas non-Hodgkin’s is the most common type of ocular lymphoma.
SICKLE CELL RETINOPATHY
Findings: This retinopathy is divided into non-proliferative and proliferative. Although neovascularization may be seen at the optic disc and the macula, proliferative sickle cell retinopathy is primarily a peripheral retinal disease that can lead to severe vision loss. Optometrists may note retinal vascular occlusions, epiretinal membrane, ischemic optic neuropathy and chorioretinal infarctions. The presence of a retinal artery occlusion in black patients younger than age 40 should raise suspicion for underlying sickle hemoglobinopathies. Although rare, retinopathy can occur in patients with sickle cell trait in the absence and presence of concomitant systemic disease, such as diabetes or hypertension.
Patients with non-proliferative retinopathy should be followed periodically, according to the level of involvement. For proliferative retinopathy, the aim is to prevent ischemic complications, particularly vitreous hemorrhages and retinal detachments. Treatment options include the use of diathermy, cryotherapy and laser photocoagulation.
Hematologic disease: Proliferative retinopathy is more characteristic of patients with sickle-hemoglobin C disease and sickle beta-thalassemia than the more severe systemic form of sickle cell anemia.
Background: The sickle cell hemoglobinopathies are an inherited group of disorders due to a structurally abnormal beta hemoglobin chain subunit. The result is formation of crescent-like, or sickle-shaped, red blood cells in response to decreased oxygen concentration or other physiological stresses. Sickle cell disease is one of the most prevalent genetic disorders in the United States, and it predominately affects individuals of African and Mediterranean descent. The four common variants include: sickle cell anemia, sickle-hemoglobin C disease, sickle beta-thalassemia and sickle cell trait. Individuals with sickle cell trait inherit one normal hemoglobin and one sickle hemoglobin-S, resulting in the AS genotype. Approximately 3 million Americans, or 9%, have sickle cell trait (HbAS) says the EBioMedicine Journal.
OUR ROLE
By staying abreast of the retinal findings associated with the hematologic diseases mentioned above, optometrists can both identify and monitor these diseases, enabling referrals to primary care physicians for definitive diagnoses and ongoing conversations with them about the patient’s condition that can benefit management. OM
