


A: You can acquire specific target measures of macular function and structure that can help you detect AMD early. This will facilitate a focused discussion of modifiable risk factors to reduce the likelihood of vision loss from AMD.
TARGET NO. 1: UNCOVER VISUAL DYSFUNCTION
The earliest onset of pathology is often signaled by a decline in visual function that precedes obvious tissue alterations. Consider using the following sensitive tools to help you detect early dysfunction:
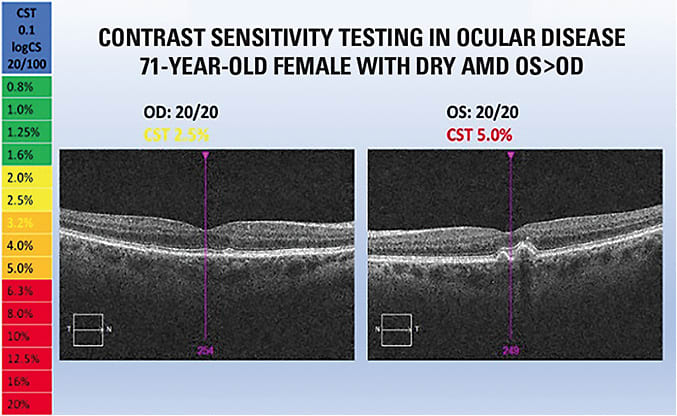
Contrast Sensitivity Testing
VA often remains normal in early AMD. However, reduced contrast sensitivity (CS) is a consistent finding in eyes that have macular drusen, making it a preferred measure to aid in identifying AMD and in understanding its real-world visual impact.1,2
Letter CS is most often assessed with the Pelli-Robson chart, which features large letters of decreasing contrast from the chart’s top to bottom. User-friendly, calibrated electronic charts also are available for efficient testing of CS, and these have been validated to match the Pelli-Robson chart.
Action step: A finding of asymmetric or suboptimal CS without other known explanation should be followed by a careful inspection of macular integrity that may lead to an earlier diagnosis of AMD.
Dark Adaptation Testing
Poor night vision is recognized as an early sign of AMD. In fact, research shows that patients who have no signs of macular disease but who have abnormal dark adaptation (DA) are twice as likely to develop early AMD over the following three-year period.3 Much less frequent causes of poor DA, such as retinal dystrophy, vitamin A deficiency (rare in industrialized countries) or zinc deficiency in patients who have liver disease, should be ruled out when DA is abnormal. Commercially available instruments measure DA.
Action step: When DA is abnormal despite the lack of fundus changes noted on exam, subclinical AMD is the likely diagnosis. In this case, carefully explain to the patient the diagnosis of subclinical AMD, and provide counseling as noted below.
Of note: DA testing also can help confirm the AMD diagnosis when equivocal fundus changes are noted, allowing for a confident patient discussion.
TARGET NO. 2: IDENTIFY STRUCTURAL ABNORMALITIES
Specific retinal changes, such as the presence of drusen or changes to RPE, can be identified in AMD. Depending on the characteristics of macular drusen and/or pigmentary irregularities, these could be considered early to classified as early to moderate AMD. Advanced AMD occurs when abnormal, leaky blood vessels or atrophic macular changes develop, often bringing significant vision loss. The potential for preventing visual disability hinges on identifying the disease at its earliest stage. The following diagnostic tests are key in this effort:
Stereo Fundus Examination
A thorough fundus exam through a dilated pupil can uncover early signs of pigmentary migration and/or drusen. However, success in finding fundus changes can be limited by cataracts, pupil size, light sensitivity, and patient non-cooperation. For example, ECPs in one study looking specifically for AMD failed to properly diagnose it 25% of the time, suggesting that retinal signs of the disease are frequently not obvious.4 Therefore, it is highly recommended that fundus examination be used in concert with the other tools described in this article to increase likelihood of early diagnosis.
Fundus Photography
High-resolution color fundus photography with red and green filters can assist in analyzing the layers of retinal tissue. This aids in the identification of signs of macular disease, including small- to large-sized drusen and areas of hypo- or hyperpigmentation consistent with AMD.
Fundus Autofluorescence
Excessive lipofuscin accumulation in the outer retina can be a sign of AMD and is readily identified with fundus autofluorescence. Areas of hypo- or hyper-fluorescence make it possible to detect macular pathology not obvious when using traditional fundus photography or other means of evaluation.
Action step for these three tests: Once fundus changes are identified with these techniques, further structural evaluation using tools, such as OCT imaging, should be ordered to help confirm the diagnosis of AMD and provide a necessary baseline.
OCT Imaging
This can confirm the size, type and extent of drusen, while ruling out macular fluid. Of note, OCT images also allow us to track progressive macular changes by comparing images over time.
Action step: Patients who have structural changes of AMD need careful monitoring for progression. This should include periodic repeat OCT, along with monocular home monitoring using the Amsler grid or an electronic device to help detect changes in macular status that may occur among visits. (For more information about take-home devices to monitor AMD, read Dr. Damon Dierker’s article “Embrace Self-Monitoring for Posterior Segment Disease” at bit.ly/OM1120SelfMonitoringDierker .)
TARGET NO. 3: UNDERSTAND RELEVANT GENETICS
It is known that genetics play a major role in risk for development of AMD. Although more than 30 genes have been associated with this complex disease, two specific loci, CFH and ARMS2, contribute more than 60% to its heredity. The presence of the high-risk variants in the CFH gene alone leads to a greater than seven-fold increase in the risk of having AMD.5
Genetic Testing
Controversy exists as to the interaction of high-risk genetic variants in patients with AMD and the use of the AREDS formula with high-dose zinc. Several studies show there are benefits for certain genotypes, but potential harm with this formula in one specific genetic profile comprising about 15% of those who have the disease. A recent study using a new data set again found this gene interaction leading to a nearly five-times increase in risk of progressing to wet AMD.6 Of interest, it is shown that certain genetic variants, certain variants within the CFH gene, also provide additional protection from both forms of late AMD when a Mediterranean diet is followed, especially in regard to fish intake.5
The role of genetic testing is likely to grow as we enter an era of customized patient care.
Family History
Research shows that when a parent has AMD, the odds that offspring will develop it over a lifespan is more than 25 times greater, while the odds are 12 times greater when a sibling is affected.7 These odds ratios are even higher when factors such as age and smoking are considered.
Action step: Consider genetic testing to better inform recommendations. It is likely that patients at greater genetic risk informed at an earlier point in the disease process will be more compliant with strategies to reduce risk. Discuss family history during each exam, and be certain to address lifestyle factors with these patients (discussed below).
TARGET NO. 4: ADDRESS MODIFIABLE RISK FACTORS
Several behaviors influence the risk of AMD onset and progression; so, patients must be encouraged to make proper lifestyle choices. AMD risk factors include:
Smoking
This is the most important modifiable risk factor, and current smokers are two to four times more likely to develop or progress in AMD compared to those who have never smoked.8 Exposure to second-hand smoke nearly doubles the risk after five years as well but, on the positive side, after 20 years of smoking cessation the risk of AMD is the same as for nonsmokers.8,9
Action step: Smoking history must be documented in the record and then addressed with an emphasis on cessation to reduce significant risk of blindness. Pharmaceutical therapy or counseling for smoking cessation should be promoted.
Macular Pigment Status
Based on several epidemiological studies, patients with the highest dietary intake of the macular carotenoids appear to be at lower risk of developing AMD.10-12 The AREDS2 study demonstrates that nutritional intervention with macular carotenoids reduces risk of wet AMD, especially in those individuals who have low dietary levels.13
Action step: Commercially available devices measure or estimate a patient’s macular pigment optical density (MPOD) at a given location, or the macular pigment optical volume (MPOV), the amount of macular pigment across a given diameter. I recommend following manufacturer guidelines for interpretation and when values are low, prescribe an increase in dietary intake of colorful fruits and vegetables or the Mediterranean diet.14 Additionally, macular carotenoid supplements can enhance macular pigment, which provides antioxidant protection, reduces inflammation and increases blue light protection to the macular tissue. (More on blue light below.)
Low Omega-3 Intake
Observational studies indicate that patients who have higher dietary levels of the long-chain omega-3 polyunsaturated fatty acids, EPA and DHA, along with increased fish intake, are at lower risk of developing AMD.15-16
Action step: A blood test, known as the omega-3 index and expressed as a percentage, can be obtained through red blood cell membrane analysis. A score above 8% is ideal, as it has been linked in numerous studies to improved cardiovascular and eye health.17-19 Once the index is known, it is easy to titrate the dose through changes in fish intake or omega-3 supplements to reach the desired omega-3 level.
Sunlight Exposure
The Beaver Dam Eye Study shows a significant association between a history of more than five hours of daily sun exposure and a 10-year incidence of early age-related maculopathy.20 Increases in retinal pigmentary changes also were noted in the greater sun exposure group. Since UV light is absorbed by the cornea and lens, it is the high-energy blue light that is of great concern with regard to the retina.
Action step: Lenses that filter blue light should be prescribed to defend against solar radiation that may contribute to retinal damage over time. Additionally, increased macular carotenoid intake enhances the strategically placed macular pigment to reduce photo-toxic effects.21
Physical Activity
Results from the Healthy Lifestyles Related to Subsequent Prevalence of Age-Related Macular Degeneration study indicate that those in the highest vs. lowest quintile of physical activity had a greater than 50% lower odds of developing any type of AMD.22 Risk for early AMD was more intricately linked to the time spent in exercise rather than the type or intensity.22
Action step: Discuss the importance of physical activity with AMD patients. Those at the lowest risk in this study engaged in moderate exercise for at least an hour per day, but setting a goal of moderate exercise 30 minutes daily for five days per week (doubled for more benefits and approved by the patient’s PCP as indicated) is consistent with the HHS/USDA recommendations.23
Systemic Health
Evidence continues to build for the importance of a holistic approach to AMD. Studies show associations of AMD with cardiovascular disease, diabetes, hypertension and increased cholesterol.24,25
Action step: Patients should be made aware of the link between general health and AMD and encouraged to comply with treatment and lifestyle recommendations for systemic health conditions.
EMPHASIZE ONGOING EYE CARE
For patients who have early AMD and for those who have disease risk factors, patient compliance to prescribed treatments, early detection and keeping a watchful eye on disease progression is key. A customized approach is best, since yearly evaluation may be adequate for some patients, while others will require more frequent monitoring.
It is ideal to check responses to nutritional intervention, primarily through repeat CS and DA testing, macular pigment measurement and appropriate blood work. Finally, patients who have macular disease should use a home monocular Amsler grid or a remote monitoring device, when qualified, to help detect changes that may occur between office visits. OM
REFERENCES
- Stangos N, Voutas S, Topouzis F, Karampatakis V. Contrast sensitivity evaluation in eyes predisposed to age-related macular degeneration and presenting normal visual acuity. Ophthalmologica. 1995;209(4):194-198.
- Roark, MW, Stringham, JM, Visual performance in the “real world”: contrast sensitivity, visual acuity, and effects of macular carotenoids. Mol. Nutr. Food Res. 2019, 63, 1801053.
- Owsley C, McGwin G Jr, Clark ME, et al. Delayed rod-mediated dark adaptation Is a functional biomarker for incident early age-related macular degeneration. Ophthalmology. 2016;123(2):344-351.
- Neely DC, Bray KJ, Huisingh CE, Clark ME, McGwin G Jr, Owsley C. Prevalence of undiagnosed age-related macular degeneration in primary eye care. JAMA Ophthalmol. 2017 Jun 1;135(6):570-575.
- Chew, EY. Age-related macular degeneration: nutrition, genes and deep learning—the LXXVI Edward Jackson Memorial Lecture. Am J Ophthalmol. 2020;217:335-347. doi: 10.1016/j.ajo.2020.05.042. Epub 2020 Jun 20.
- Kaufman SR, Yoganathan P, Small KW, Rusia D. Genetics and age-related eye disease study formulation interaction in neovascular age-related macular degeneration. Journal of VitreoRetinal Diseases. 2020: DOI: 10.1177/2474126420941713.
- Shahid H, Khan JC, Cipriani V, et al. Age-related macular degeneration: the importance of family history as a risk factor Br J Ophthalmol. 2012;96:427-431 doi: 10.1136/bjophthalmol-2011-300193.
- Velilla S, Garcia-Media JJ, Garcia-Layanna A, et al. Smoking and age-related macular degeneration: review and update. J Ophthalmol. 2013:895147. doi:10.1155/2013/895147.
- Khan JC, Thurlby DA, Shahid H, et al. Smoking and age-related macular degeneration: the number of pack years of cigarette smoking is a major determinant of risk for both geographic atrophy and choroidal neovascularisation. Br J Ophthalmol. 2006 Jan;90(1):75-80. doi: 10.1136/bjo.2005.073643.
- Seddon JM, Ajani UA, Sperduto RD, et al. Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. Eye Disease Case-Control Study Group. JAMA. 1994;272(18):1413-20.
- Tan JS, Wang JJ, Flood V, Rochtchina E, Smith W, Mitchell P. Dietary antioxidants and the long-term incidence of age-related macular degeneration. Ophthalmol. 2008;115(2):334-41. doi: 10.1016/j.ophtha.2007.03.083. Epub 2007 Jul 30.
- Bone RA, Landrum JT, Mayne ST, Gomez CM, Tibor SE, Twaroska EE. Macular pigment in donor eyes with and without AMD: a case-control study. Invest Ophthalmol Vis Sci. 2001;42(1):235-240.
- Chew, EY. Secondary analyses of the effects of lutein/zeaxanthin on age-related macular degeneration progression. JAMA Ophthalmol. 2014;132(2):142-149. doi:10.1001/jamaophthalmol.2013.7376.
- Merle, BMJ, Colijin JM, Cougnard-Gregoire A, et al. Mediterranean diet and incidence of advanced age-related macular degeneration: The EYE-RISK Consortium. Ophthalmology. 2019;126(3):381-390. doi: 10.1016/j.ophtha.2018.08.006. Epub 2018 Aug 13.
- Christen, WG, Schaumberg DA, Glynn RJ, Buring JE. Dietary ω-3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch Ophthalmol. 2011;129(7): 921–929. Published online 2011 Mar 14. doi: 10.1001/archophthalmol.2011.34.
- Chong, EW, Kreis AJ, Wong TY, Simpson JA, Guymer RH. Dietary omega-3 fatty acid and fish intake in the primary prevention of age-related macular degeneration: a systematic review and meta-analysis. Arch Ophthalmol. 2008;126(6):826-33. doi: 10.1001/archopht.126.6.826.
- Harris WS and Von Schacky C. The Omega-3 Index: a new risk factor for death from coronary heart disease? Prev Med. 2004;39:212-220. doi:10.1016/j.ypmed.2004.02.030.
- Harris WS, Gobbo LD, Tintle NL. The Omega-3 Index and relative risk for coronary heart disease mortality: Estimation from 10 cohort studies. Atherosclerosis. 2017;262:51-54.
- Souied EH, Delcourt C, Querques G, et al. Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: the nutritional AMD treatment 2 study. Ophthalmology. 2013; 120(8):1619-1631. doi: 10.1016/j.ophtha.2013.01.005. Epub 2013 Feb 8.
- Tomany SC, Cruickshanks KJ, Klein R, Klein BE, Knudtson MD. Sunlight and the 10-year incidence of age-related maculopathy: the Beaver Dam Eye Study. Arch Ophthalmol. 2004;122(5):750-757. doi:10.1001/archopht.122.5.750.
- Snodderly DM. Evidence for protection against age-related macular degeneration by carotenoids and antioxidant vitamins. Am J Clin Nutr. 1995;62(6):S1448-S1461. doi: 10.1093/ajcn/62.6.1448S.
- Mares, JA, Voland RP, Sondel SA, et al. Healthy lifestyles related to subsequent prevalence of age-related macular degeneration. Arch Ophthalmol. 2011 Apr;129(4):470-80. doi: 10.1001/archophthalmol.2010.314. Epub 2010 Dec 13.
- 2015-2020 Dietary Guidelines for Americans. U.S. Department of Health and Human Services Website. Accessed Nov. 9. https://health.gov/our-work/food-nutrition/2015-2020-dietary-guidelines .
- Vassilev ZP, Ruigomez A, Soriano-Gabarro M, Rodriguez LAG. Diabetes, cardiovascular morbidity, and risk of age-related macular degeneration in a primary care population. Invest Ophthalmol Vis Sci. 2015;56(3):1585–1592. doi: 10.1167/iovs.14-16271.
- Cheung CMG and Wong TY. Is age-related macular degeneration a manifestation of systemic disease? New prospects for early intervention and treatment. J Intern Med. 2014;276(2):140-53. doi: 10.1111/joim.12227. Epub 2014 Mar 21.
