


Three tricks from this technological treat
OCTOBER HOSTS HALLOWEEN, which is a time of tricks and treats (even though this year’s celebration will likely occur within our own social-distancing circles). With that said, this month’s column will focus on three tricks of employing OCT in relation to glaucoma.
1 LOOK FOR AREAS OF RELATIVE THINNING
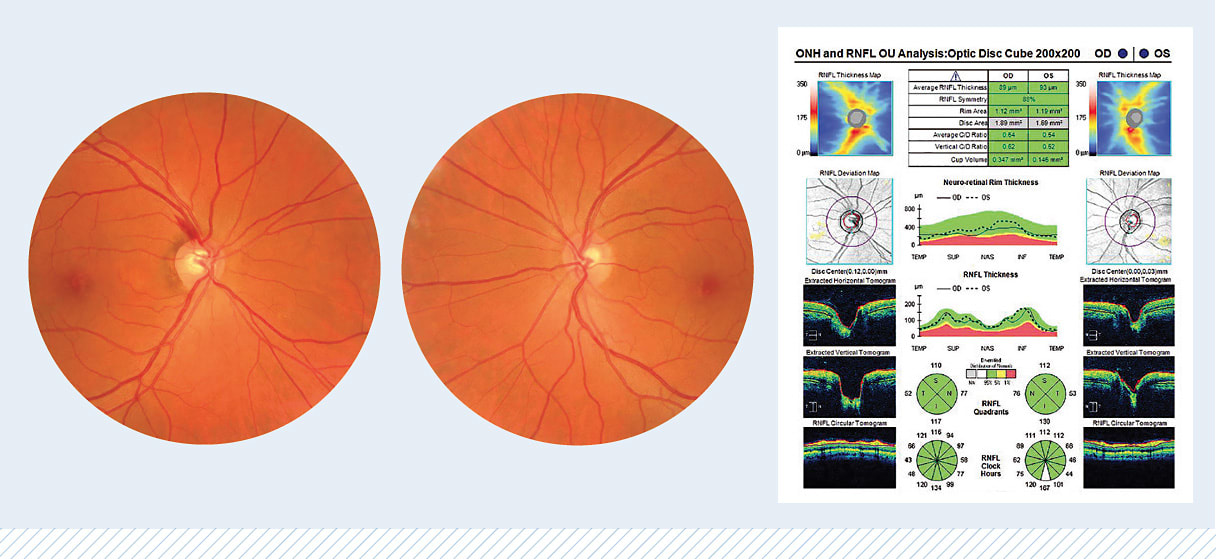
Focal areas of relative retinal nerve fiber layer (RNFL) thinning on OCT analysis are clues that may not seem clinically significant but, when considered in the context of the clinical exam, add confidence to our concerns and certainty regarding testing, as shown in the fundus images and OCT printout below. So, OCT will not necessarily show glaucomatous disc hemorrhages, but it will show associated thinning concurrently or months down the road following the disc hemorrhage. Structure-structure correlation adds confirmation when we are diagnosing glaucoma or suspecting progression.
2 WATCH FOR SCANNING ANOMALIES
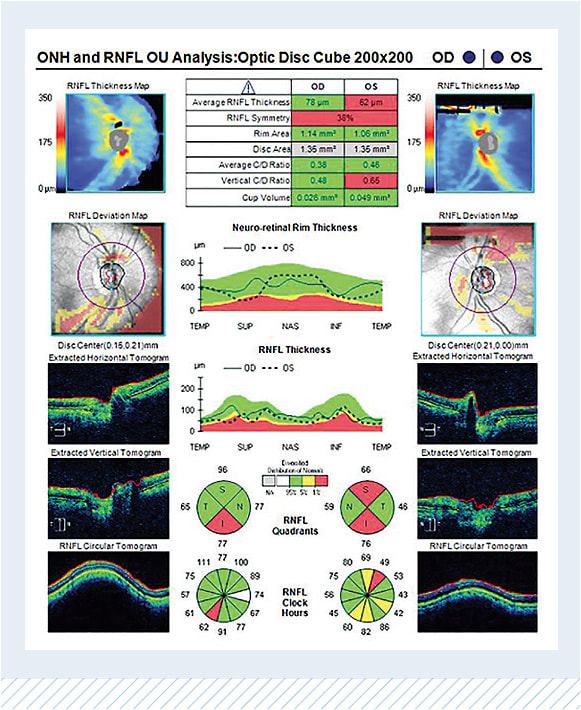
After ensuring the analysis printout correlates with the clinical exam — and is indeed the correct patient with the correct age — we should watch for scanning anomalies, which appear as horizontal black boxes with corresponding non-physiological RNFL loss or media opacities, such as posterior vitreous detachments. These items can cause focal dark patches. If these anomalies are within the scanning circle, the analysis will show associated artificial relative RNFL loss — literal black masks, which may hide the true findings. Other important variables that influence the reliability of the scan include decentration, moderate/high hyperopia or myopia outside the reference database range (therefore caution when interpreting results), cyclotorsion/head tilt and decreased signal strength with segmentation errors due to ocular conditions, such as surface disease (very common in dry eye disease patients) and cataracts.1
3 JUXTAPOSE PREVIOUS SCANS
Compare previous scans of similar signal strength while focusing on the inferior and superior temporal sectors in early glaucoma or the deepening/broadening of known defects in moderate glaucoma. Individual comparison of scans is helpful, but don’t forget to use the guided progression analysis algorithms and let the computer do the work where/when possible. With such careful comparison, we should watch for hot spots of possible progression and repeat testing sooner as indicated.
TRICK AND TREAT
In the Halloween spirit, let’s focus on the tricks of using OCT, while enjoying the treat of this advanced, complimentary technology. OM
REFERENCE
- Chen JJ, Kardon RH. Avoiding Clinical Misinterpretation and Artifacts of Optical Coherence Tomography Analysis of the Optic Nerve, Retinal Nerve Fiber Layer, and Ganglion Cell Layer. J Neuroophthalmol. 2016;36(4):417–438
