


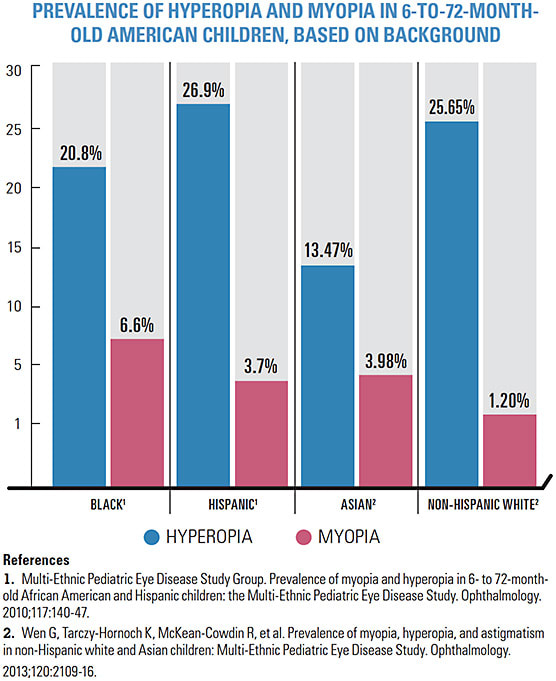
While myopia management receives a lot of attention these days, hyperopia is, interestingly, more common in the U.S. population than myopia.1 Population studies of the United States estimate the prevalence of farsightedness greater than or equal to 3.00 D to be between 5% and 10% in those older than 40.2,3 In the younger population, most newborns are born with an average of 3.00 D of hyperopia, and most decline to about 1.00 D by 1 year of age.4 However, 20% of children younger than age 5 are estimated to remain at 2.00 D or more of hyperopia, which increases their risk for the development of strabismus and amblyopia.5,6
We, as optometrists, must be ready to manage this sizable population using all the options available. Below, we review these hyperopia treatment options available and how to pair them to the right patients.
SPECTACLE LENSES
The potential for amblyopia in young hyperopic patients is always the primary concern, as amblyogenic risk is increased when both eyes have greater than 5.00 D of hyperopia and when the difference between the eyes is greater than 1.00 D.7 To reduce risk of vision loss, both the American Academy of Ophthalmology (AAO) and the American Optometric Association (AOA) recommend correction by spectacle lenses or contact lenses in these patients to reduce the risk of lifelong loss of vision.
The AAO’s recommendations, based on the 2017 published practice guidelines, are more specific than the AOA’s guidelines, which recommend spectacle correction for children ages 2 to 3 with hyperopia of 4.50 D or more, and for children ages 3 to 4 with hyperopia of 3.50 D or more. However, the AAO has no specific prescribing recommendations for those older than age 4.8 However, in a 2004 survey of prescribing habits, 67% of optometrists and 42% of pediatric ophthalmologists reported they would prescribe spectacle lenses for 4-year-old children who have asymptomatic hyperopia greater than 3.00 D.9
In recommending spectacle lenses for both children and adults who have hyperopia, consider accommodative and binocular vision status. If esotropia is present in children who have hyperopia, the full amount of hyperopia correction should be prescribed. However, if accommodation and binocular vision problems are not present and the hyperopia is moderate (3.00 D to 6.00 D) or high (greater than 6.00 D) and the patient has reduced visual acuity, spectacle lenses are recommended and the total amount of hyperopia correction can be reduced 1.00 D to 3.00 D to preserve emmetropization.8
As for adults, sometimes it can be tricky to find the right prescription for those who have hyperopia who have been visually happy and asymptomatic all their lives and now feel end-of-the-day visual fatigue due to fading accommodation. Generally, it’s best to start with very low amounts of hyperopic correction in either glasses or contact lenses and gradually work upward year after year.
Patient Case – Caring for a Hyperopic Adult
SOMETIMES, HYPEROPIC ADULTS, ESPECIALLY THOSE WITH ADDITIONAL PRESBYOPIA, CAN BE THE MOST DIFFICULT PATIENTS TO SATISFY. A RECENT PATIENT OF MINE ILLUSTRATES THIS POINT.
Patient TA, a 49-year-old female, presented for her first eye exam in over a decade. Her main complaint was blurry vision while driving or while working on her computer or phone. She used a +3.00 D OTC reader for near work. Her uncorrected VA was 20/30 OD and 20/40 OS. I prescribed +1.50-0.25x103 OD and +1.75 with an add of +1.50. Four months later, she came back to our office because her distance vision was blurry in the new lenses, but she liked how well she could see at near. She also expressed wanting a pair of glasses just for the computer. I adjusted her prescription slightly by reducing her plus for distance, which alleviated the blur in the phoropter, and prescribed a separate computer progressive lens. Her final power was +1.25-0.25x103 OD and +1.25 OS with an ADD of +2.00.
One year later, TA came back for her annual exam and was no longer wearing the most recently prescribed progressive addition lens. Instead, she was wearing the computer progressive lens nearly full-time because it provided the best vision. The computer pair was +2.50-0.25x103 OD and +2.50 OS with an add of +1.25. She was also interested in contact lenses, so I recommended a silicone hydrogel daily disposable lens. Her final prescription was +2.25-0.50x103 OD and +2.25 OS with an add of +2.00 D. She successfully fit into a silicone hydrogel daily disposable multifocal lens at +2.00/HI OD and +2.25/HI OS.
Ten months after our last appointment, despite purchasing new glasses and a year’s supply of contact lenses and being seemingly satisfied, TA arrived at our office with a complaint of eye discomfort. Unknown to our office, TA had LASIK surgery in both eyes one month earlier because she got tired of wearing glasses and contact lenses. Indeed, she was happier with her vision, now 20/20 OD and 20/30 OS uncorrected, with a manifest refraction of +1.00-0.75x095 OD and pl-1.00x115 OS. However, now she was experiencing dry eye.
In my assessment, our patient had adequate results with LASIK correction of her hyperopia. So, we offered a prescription for glasses, which she denied, and we went to work treating her residual dry eye.
Sometimes, even after we’ve used traditional means of refractive correction, surgical options can surprise and surpass our expectations.
CONTACT LENSES
Contact lenses, like spectacle lenses, are a good option for hyperopic patients young and old. Most contact lenses have ranges of hyperopia correction up to +6.00 D, while only a handful of lenses go up to +10.00 D.
A recent study on safety of pediatric contact lens wear showed a greater incidence of contact lens adverse events in children ages 13 and older vs. children ages 8 to 12, showing that fitting patients in contact lenses at those young ages can be a safe alternative to spectacle lenses.10
Contact lenses have several advantages, including improved cosmesis, reduction of aniseikonia when present, and elimination of prismatic imbalance.7 Hyperopic adults, especially those whose latent hyperopia is gradually being manifested, are great candidates for contact lenses due to their consistently changing refraction. These patients may require multifocal lenses even in pre-presbyopic stages in their mid to late 30s.
In addition to soft contact lenses, gas permeable, scleral, and orthokeratology lenses are readily available for patients with hyperopia.
SURGICAL OPTIONS
Most excimer lasers are approved for treatment of up to +5.00 D to +6.00 D of hyperopia.11 However, I’d advise surgeons to be more judicious in recommending laser correction for hyperopia.
The ideal candidate tends to be younger than 50 years old, with less than +3.00 D of hyperopia with or without astigmatism.12 However, hyperopia correlates to the highest rate of LASIK retreatment. Further, due to the large ablation zone needed for treatment, patients are often unhappy with subsequent optical aberrations, such as glare and halos.13
When patients are 50 years old or older and/or have greater than +3.00 D of hyperopia, refractive lens exchange (RLE) or clear lens exchange is a good and growing option.12 RLE is essentially cataract surgery without the cataract. The risks are the same as any cataract surgery with the disadvantages being related to the loss of accommodation.
SETTING PATIENT EXPECTATIONS
No matter what treatment we recommend for our hyperopic patients, we must set clear expectations. If prescribing for children, we must emphasize to parents how prescription lenses will assist proper visual system development. So even if 20/20 vision is not achieved immediately with their child, they understand the importance of vision correction and will more likely adhere to our recommendations. Adults often have unrealistic expectations of getting their vision back to where it used to be. This requires extra patience on our part to both educate and sometimes trial and error options that could work best for them. The result of a satisfied patient, though, is well worth the effort. OM
MORE ON REFRACTIVE ERRORS



HOW DO I DIAGNOSE AND MANAGE AMBLYOPIA?
WHAT ARE THE TREATMENT OPTIONS FOR PRESBYOPIA?
WHAT ARE THE REFRACTIVE CORRECTION OPTIONS FOR GLAUCOMA PATIENTS?
REFERENCES
- Diniz D, Irochima F, Schor, P. Optics of the Human Eye. In: Yanoff M, Duker JS, eds. Ophthalmology. 5th ed. Philadelphia, PA: Elsevier; 2019:2.2, 26-37.
- Kempen JH, Mitchell P, Lee KE, et al. The prevalence of refractive errors among adults in the United States, Western Europe, and Australia. Arch Ophthalmol. 2004;122(4):495-505.
- Vitale S, Ellwein L, Cotch MF, et al. Prevalence of refractive error in the United States, 1999-2004. Arch Ophthalmol. 2008;126(8):1111-9.
- Saunders KJ. Early refractive development in humans. Surv Ophthalmol. 1995;40(3):207-16.
- Multi-Ethnic Pediatric Eye Disease Study Group. Prevalence of myopia and hyperopia in 6- to 72-month-old African American and Hispanic children: the Multi-Ethnic Pediatric Eye Disease Study. Ophthalmology. 2010;117:140-47.
- Wen G, Tarczy-Hornoch K, McKean-Cowdin R, et al. Prevalence of myopia, hyperopia, and astigmatism in non-Hispanic white and Asian children: Multi-Ethnic Pediatric Eye Disease Study. Ophthalmology. 2013;120:2109-16.
- Rouse MW, Cooper JS, Cotter SA, et al. Optometric Clinical Practice Guideline: Care of the Patient with Amblyopia. St. Louis, MO: American Optometric Association; 2004.
- Pediatric Eye Evaluations PPP - 2017 - American Academy of Ophthalmology Pediatric Ophthalmology. American Academy of Ophthalmology. https://bit.ly/AAOPPP2017 . Published November 2017. Accessed Nov. 8, 2022.
- Lyons SA, Jones LA, Walline JJ, et al. A survey of clinical prescribing philosophies for hyperopia. Optom Vis Sci. 2004 Apr;81(4):233-7.
- Chalmers RL, McNally JJ, Chamberlain P, Keay L. Adverse event rates in the retrospective cohort study of safety of paediatric soft contact lens wear: the ReCSS study. Ophthalmic Physiol Opt. 2021;41(1):84-92.
- Chuck RS, Jacobs DS, Lee JK, et al. Refractive Errors & Refractive Surgery Preferred Practice Pattern. Ophthalmology. 2018;125(1):P1-P104.
- McKinney S. Finding Hyperopia’s Surgical Sweet Spot. Review of Ophthalmology. March 7, 2020.
- Frings A, Intert E, Steinberg J, et al. Hyperopia shows the strongest association with LASIK retreatment. Acta Ophthalmol. 2018;96(3): e404–e404.
