


Fast and deep. That’s the easiest way to describe Swept Source (single wavelength laser) SS-OCT. How fast? Some 100,000 axial scans per second, reports Topcon, one manufacturer of the technology. How deep? A total of 1,050 nm to 1,060 nm wavelengths — depending on the manufacturer of the technology.
Although SS-OCT is new to the profession, here’s an overview of the technology and what eye care experts have experienced.
THE DEVICES
Currently, two SS-OCT devices have FDA clearance: the DRI OCT Triton (Topcon) and the PLEX Elite 9000 (Zeiss). Topcon’s Triton received FDA 501(k) clearance in January. Zeiss received clearance for both OCT and OCT angiography (OCTA) applications of the Plex Elite SS-OCT device in 2016.
The Triton device is commercially available. Zeiss is currently targeting clinical researchers for its commercial PLEX Elite SS-OCT through membership in the Advanced Retina Imaging (ARI) Network. The ARI Network is a global consortium of clinical researchers.
Philip J. Rosenfeld M.D., Ph.D., and chairman of the ARI Network, explains: “This collaboration between the retina experts in the ARI Network and the engineers and scientists at Zeiss is vital to the advancement of retinal and choroidal imaging and scientific discovery.”
According to Zeiss: “Due to its longer wavelength and larger scanning depth, SS-OCT, when combined with OCTA, can visualize changes in choroidal microvasculature. SS-OCT technology and clinical research are both rapidly evolving, and clear understanding of the value of SS-OCT in daily clinical practice is only beginning to emerge.” (See http://bit.ly/2uOVYDk for more information on SD-OCTA, an important tool for visualizing microvasculature changes in the retina, which are observed in diseases such as AMD and diabetic retinopathy.)
THE CAPABILITIES
Carl Glittenberg, M.D., F.E.B.O., and global medical director at Topcon, says the longer wavelength light source captures the vitreous, retina and choroid in one image:
“The longer wavelength reduces risks of light attenuation by cataract and vitreous opacity, enabling [it] to image through media opacities,” Dr. Glittenberg explains.
This light wavelength also may benefit patient concentration by providing a fixation target, which may reduce eye movement, he adds.
“This supports a more efficient workflow for the practice and [decreases] patient wait times by reducing re-scan,” Glittenberg says.
The DRI OCT Triton features a 1,050 nm wavelength light source.
Michael Chaglasian, O.D., associate professor at Illinois College of Optometry and chief of staff of the college’s Illinois Eye Institute, says, “I particularly like the widefield 12 mm x 9 mm scan. I can see the macula and the disc in the same scan. And with widefield outside the macula region, you can look at more peripheral retinal lesions.”
The device also includes fundus imaging so that, “in a single view, you get the color photograph and the OCT,” says Dr. Chaglasian. “You can say to the patient, ‘Here’s what I saw in the back of the eye. And here’s a cross-section of that lesion in great detail. This is how I know you have diabetic retinopathy.’”
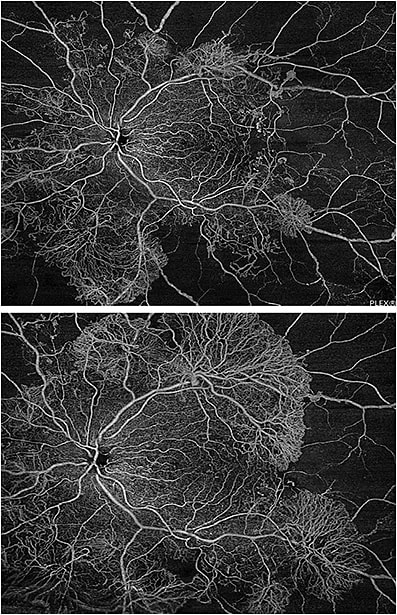
The PLEX Elite, with OCT and OCTA capability, has a 1,060 nm wavelength, allowing the viewer to see past the retinal pigment epithelium to visualize the choriocapillaris, choroid and sclera, according to Investigative Ophthalmology & Visual Science. The Plex Elite outputs 12 mm x 12 mm single shot OCT and OCTA scans for an ultra-wide view.
PRACTICE EXPERIENCES
Anthony Clark, O.D., a principal owner and chief medical officer of Triangle Optometry, a 16-clinic private practice in North Carolina, explains his experience with the technology:
“You can see more layers at the same time, and then you can separate them out. And, even things like patient eye movements don’t degrade the image.”
Additionally, Dr. Clark says:
“It offers the opportunity to see pathology early and not to just say something is abnormal, but what is abnormal about it…rather than optometrists always just seeing something and referring it out.”
Dr. Clark says OCT, in general, helps the practitioner to identify diseases earlier and more accurately. With SS-OCT and the benefit of imaging through the posterior segment you are able to identify early disease states, such as AMD and diabetic retinopathy.
Jay Haynie, O.D., who is in private practice in Tacoma, Wash., adds that the images can aid with patient compliance:
“With retinal diseases, such as AMD or diabetic retinopathy, patients may not always report improved, subjective vision with treatment,” he says. “However, OCT imaging can reassure the patient of their conical response to treatment. Demonstrating less sub-retinal fluid or macular edema with the images will often encourage the patient to maintain the advised treatment regimen. The higher image quality with SS-OCT is very valuable.”
There are practice management benefits from the technology as well, say those interviewed:
“In a busy clinical setting, the ability to achieve adequate visualization of the posterior segment is often critical,” says Dr. Haynie. “SS-OCT allows us to do that on a more efficient level, eliminating the need to achieve adequate pupil dilation in some of our patients.”
This translates to meeting the needs of more patients, says Dr. Chaglasian.
“You can more reliably acquire high-quality images on a larger percentage of patients without the artifacts that we would see with SD,” says Dr. Chaglasian. “Cataracts don’t get in the way. Small pupils aren’t such an issue. The debris in the vitreous doesn’t get in the way.”

The technology is also a valuable for imaging highly myopic patients, Dr. Chaglasian adds.
According to a 2016 study published in the Pakistan Journal of Ophthalmology, SS-OCT is beneficial in assisting clinicians in gaining a clear picture of the retina in those patients who have mild to moderate opacification caused by cataract.
Regarding workflow, a system that combines diagnostic capabilities can reduce “the need to move patients from instrument to instrument and, thus, improving exam time and patient comfort,” says Dr. Clark.
WHAT’S NEXT?
There is still a learning curve ahead for most optometrists.
“Many of us didn’t train on OCT technology, so we’re learning it,” says Dr. Chaglasian.
The profession as a whole also is still learning how this technology will fit in day-to-day practice. Improved visualization of the vitreous, retina, choroid and sclera, increased scan speeds and deeper tissue penetration all have their benefits. A study in March’s Current Ophthalmology Reports reveals that, “SS-OCT is an exciting new technology offering enhanced visualization of ocular structures. However, its everyday clinical utility remains unclear.”
The future of OCT technology is bright; clinicians will continue to see how the technology works its way into everyday clinical practice. OM