


New pharmaceutical agents, sustained-release delivery systems, biologic therapies, and presbyopia treatments are moving the ophthalmic therapeutic market toward mechanism-based treatment selection, reduced preservative exposure, and delivery platforms that are designed to improve adherence and reduce treatment burden, said Mitch Ibach, OD, FAAO, and Jake Lang, OD, FAAO, in their “Drops, Drugs, and Delivery: What’s New in Ophthalmic Therapeutics” presentation at Optometry’s Meeting 2026 in Phoenix.
Conventional topical therapies have several longstanding limitations, they explained. Less than 5% of a topical ophthalmic dose reaches intraocular targets, and much of the medication is lost through drainage and systemic absorption. Adherence also declines significantly as treatment complexity increases, particularly among patients who use 3 or more medications. Further, preservatives such as benzalkonium chloride can damage goblet cells and destabilize the tear film, which contributes to ocular surface disease.
Takeaways From Drs. Ibach and Lang:
-
Treat the mechanism, not just the diagnosis because phenotype-matched therapy outperforms empirical escalation across dye eye, glaucoma, presbyopia, and immune-mediated and inflammatory eye disease.
-
Reduce preservative and drop burdens. Sustained-release and preservative-free options now exist for most therapeutic classes, which improves surface toxicity risk with drops that contain preservatives.
-
Use delivery innovation to improve adherence. Delivery format is a therapeutic decision, not just a convenience, because a drug that isn’t taken doesn’t work.
-
Stay current. Therapeutics are changing quickly. Approvals in 2025 reshaped dry eye, presbyopia, and glaucoma treatment, and we can expect the 2026 pipeline and beyond to stay just as active.
They then introduced a few guiding principles:
-
Sequencing matters; the order in which therapies are introduced affects both efficacy and tolerability.
-
A drug won’t work if patients don’t take it, which means delivery innovation is adherence innovation.
-
Ocular surface health is a prerequisite for all topical drug delivery.
“The new goal of ophthalmic drug delivery is the right drug acting on the right target through the right delivery route, with the lowest possible patient burden,” they said, and further explained that innovation pathways are now focused on preservative-free forms of drugs, sustained release delivery, new targets, and systemic control. “Each pathway addresses a distinct failure mode of conventional therapy. Together, they represent a shift from reactive symptom management to proactive, mechanism-matched, lower-burden care. These pathways are not mutually exclusive—the most effective patient strategies often combine 2 or more approaches.”
With both of these limitations and principles in mind, Drs. Ibach and Lang reviewed the major innovations in dry eye, glaucoma, biologics and immune-mediated disease (ie, noninfectious uveitis, scleritis, Behçet disease, ocular graft vs host disease, and severe treatment refractory ocular surface disease), and presbyopia, as well as how fellow ODs can integrate them into practice.
Dry Eye Therapy Becomes More Phenotype-Specific
The presentation emphasized a shift from empirical treatment sequencing to phenotype-driven management of dry eye disease. Aqueous-deficient dry eye can be targeted with tear secretagogues and TRPM8 agonists; evaporative dry eye and meibomian gland dysfunction can be targeted with antievaporative agents and lipid layer therapy; inflammatory dry eye can be targeted with cyclosporine, lifitegrast, and reactive aldehyde inhibitors; and neurosensory dry eye can now be targeted with neuropeptide and receptor-target approaches. Drs. Ibach and Lang reviewed available therapies, as well as their clinical trial data, and clinical pearls:
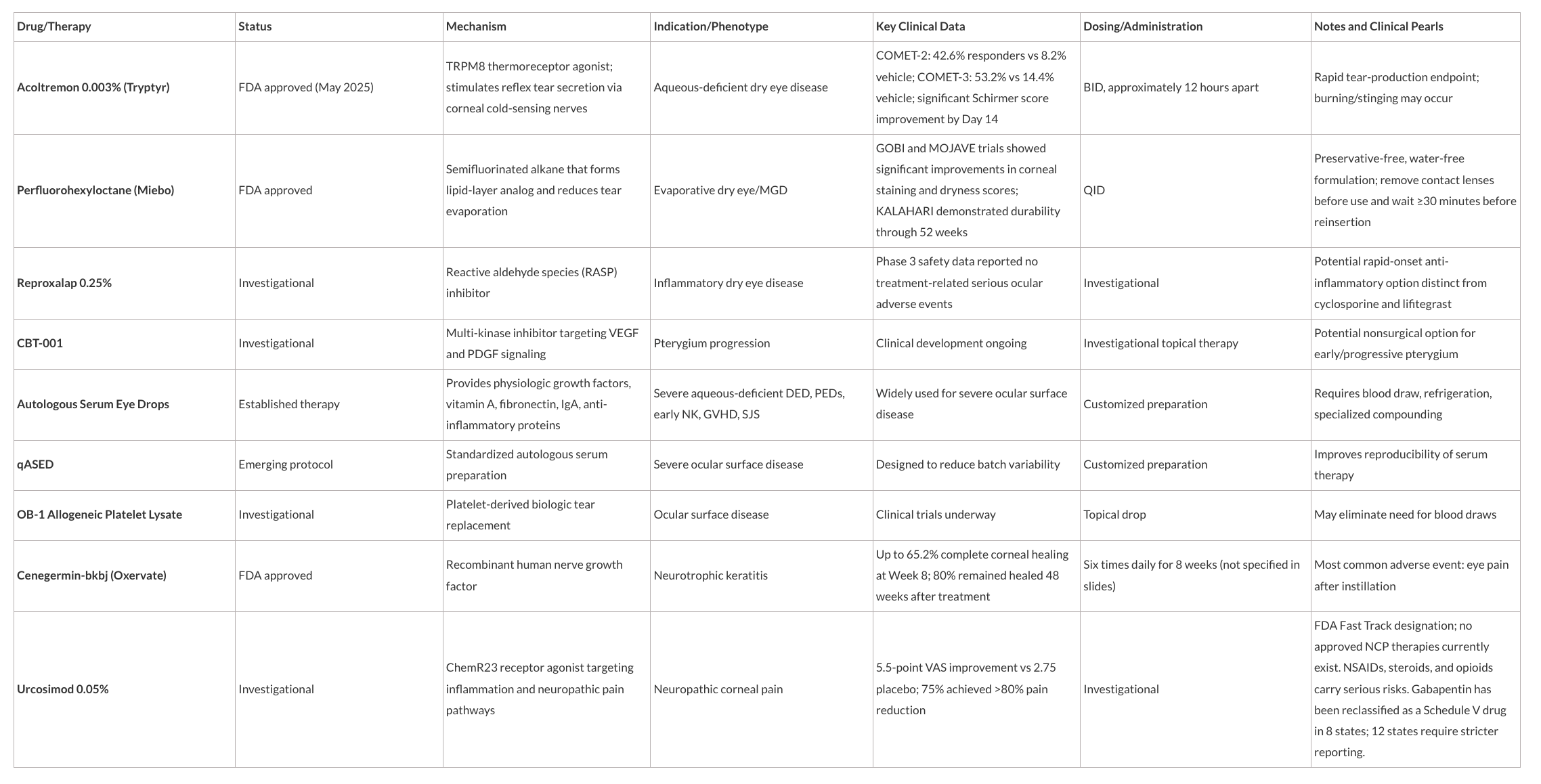
“The treatment space in dry eye has become much more cause-and-effect driven,” Dr. Ibach told OM. We try to diagnose the subtype of dry eye, or the causative factors, and then directly treat them."
Glaucoma Management Moves Beyond Bottles
"In glaucoma, we continue to prioritize lessening medication burden by using fixed-dose combination drops, drops with multiple mechanisms of action, and preservative-free drop formulations—all aimed at decreasing noncompliance caused by the high volume of drops,” Dr. Ibach added in a conversation with OM. He and Dr. Lang presented information on the following therapies:
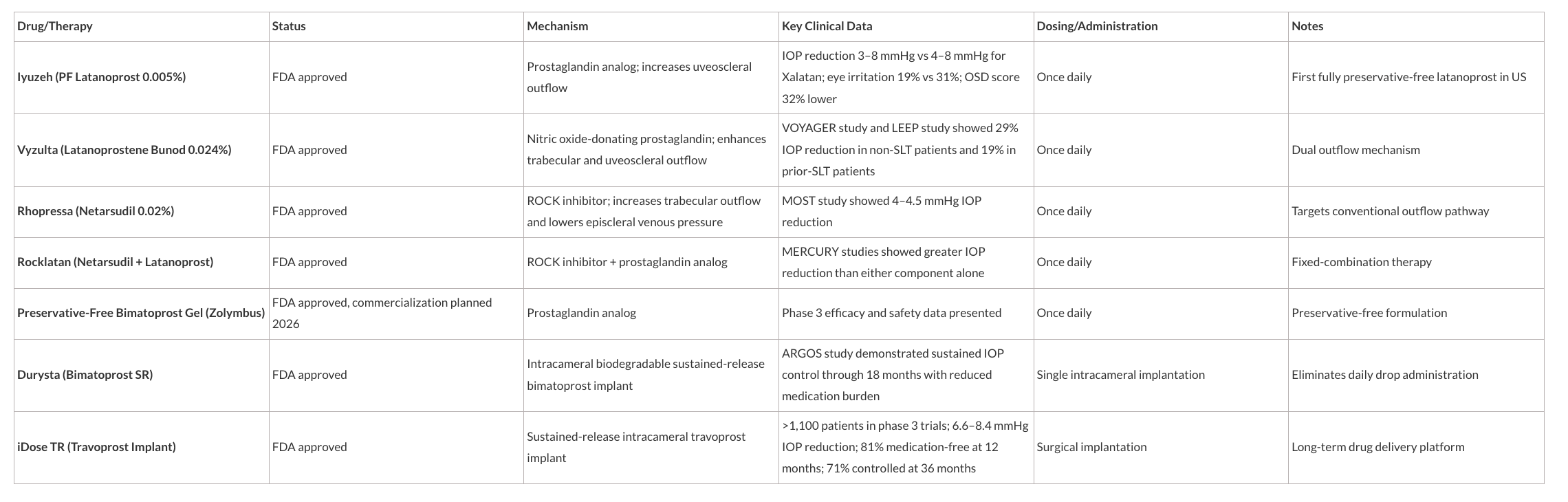
Four questions from the postoperative management discussion were drop routines, how to determine whether an implant is empty/ if treatment escalation is needed, how to titrate medications, and whether Durysta can be repeated.
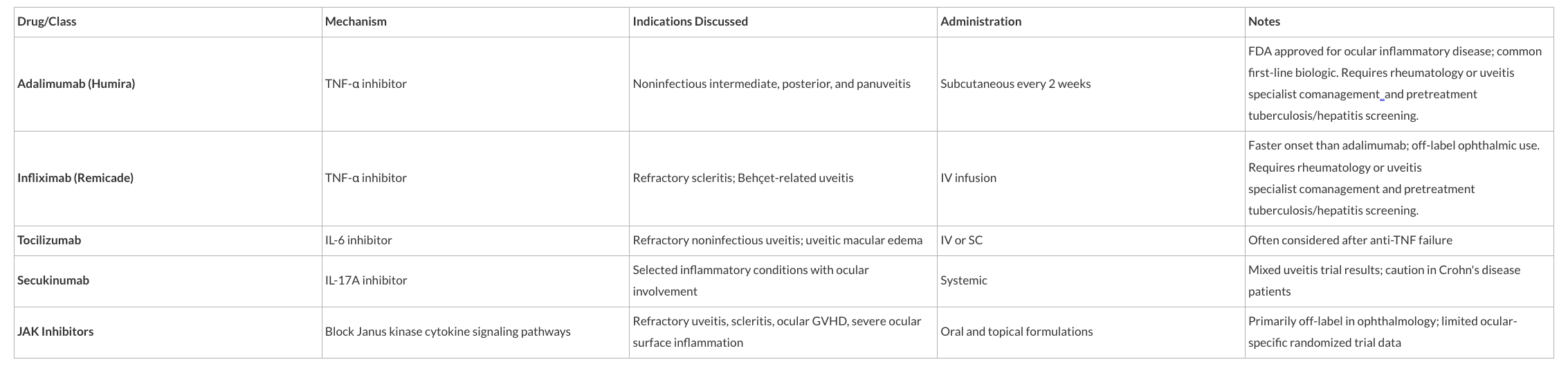
Biologics Expand Options for Ocular Inflammatory Disease
“Steroid-sparing systemic therapy is no longer a subspecialty-only tool,” Drs. Ibach and Lang said in the presentation. “It belongs in the working vocabulary of every comprehensive eyecare clinician managing chronic inflammation.” They described how steroid-sparing therapy reduces corticosteroid exposure and its long-term sequelae in chronic uveitis and inflammatory disease. Systemic inflammatory control addresses upstream immune dysregulation that topical therapy cannot reach, which is essential in Behçet disease, ocular graft vs host disease, and scleritis.
“Biologics demand diagnostic precision,” Drs. Ibach and Lang noted. “The wrong mechanism for the wrong diagnosis risks treatment failure or disease exacerbation. Comanagement with rheumatology or a uveitis subspecialist is standard of care.” The medications they discussed were:
Presbyopia Drop Market Expands
Understanding the tradeoffs is the key to successful patient selection with pharmacologic miosis as a near-vision strategy, Drs. Ibach and Lang said. While it improves depth of focus by reducing the pupil aperture and offers improved near visual acuity without requiring spectacles, the pinhole effect does not address the underlying loss of crystalline lens accommodation, they explained. Other risks include head and brow ache, possible retinal detachment, induced myopic shift, and dim vision reduction. “The clinical challenge is to identify patients whose near-vision benefits outweighs their tolerance of the side effect profile and whose lifestyle accommodates dose timing.” They discussed the following therapies:

“Your patients will ask about these drugs—often before they understand them. Your job is to translate mechanism into meaning and evidence into decisions,” Drs. Ibach and Lang concluded.
Disclosures:
Dr. Ibach is a consultant and speaker for Alcon, Bausch Health, Dompe, and Glaukos. He is a consultant for AbbVie, C-Light Tech, iCare, Orasis, Reichert, Tarsus, Thea, and Zeiss, and he is a shareholder for Balance Ophthalmics.
Dr, Lang has financial disclosures for AbbVie, Aerie,Alcon, Aldeyra, Amgen, AOS,AscuelaTech, Astra Zenica, Avellino, Bausch+Lomb, Dompe, Envision Biomedical, Horizon, Kala, Nordic Pharmaceuticals, Novartis, Ophthalmic Resource Partners, Orasis, ScienceBased Health, Scope, Sight Sciences, Sun Pharma, Tarsus, Thea, TenPoint, Visus-Oyster Point, Trukera, and Zeiss.