


Every practicing clinician has experienced cases where it seems no correct answer exists. It’s the gray area of medicine—the place most cases lie. It is vital that the clinician gather as much data as possible to have comprehensive conversations with the patient as together they decide on the best future management. This case report will discuss a 15-year-old male patient who presented on referral for progressive keratoconus that was worse in the right eye than in the left. Due to the condition of his right cornea, it was vital that the risks and benefits of epithelium-off corneal crosslinking were considered.
Case Report
A 15-year-old male patient was referred for a corneal crosslinking evaluation to treat his bilateral progressive keratoconus, which was worse in the right eye than in the left. The patient’s spectacle-corrected visual acuity (VA) was 20/200 and 20/20 in the right and left eye, respectively, and 20/20 with both eyes together. Extraocular motility, confrontation fields, and pupil testing were all unremarkable. Anterior segment examination revealed unstable keratoconus in both eyes. The right eye showed significant inferior corneal thinning and steepening, Vogt’s striae, noncentral corneal scarring, and a Fleischer’s ring as shown in Figure 1. No visible signs of keratoconus were present on anterior segment examination in the left eye.

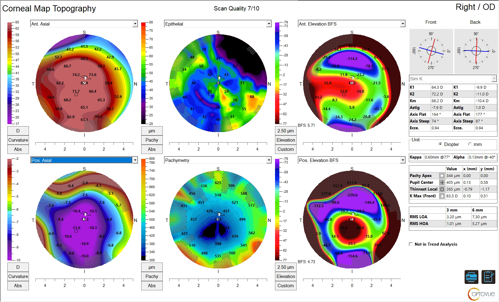
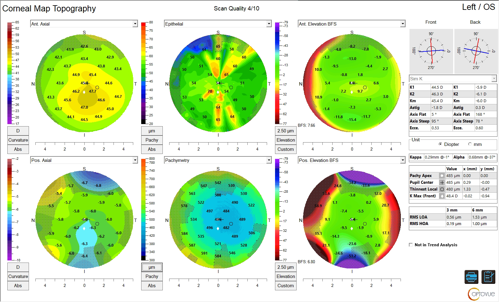
Corneal tomography scans were performed in both eyes. Tomography scans of the right eye revealed significant inferior corneal thinning with adjacent steepening. Inferior elevation of the posterior and anterior corneal surfaces was obvious, and a maximum keratometry value of 83 D confirmed the severe keratoconus in this eye (Figure 2). Tomography of the left eye showed early signs of keratoconus including inferiorly displaced corneal thinning, asymmetric corneal astigmatism, and moderate posterior surface elevation overlying the thinnest corneal point (Figure 3).
The scans in both eyes also depicted progression of both corneas from the prior corneal tomography scans, with corneal thinning of ~10% OS and 1 D of corneal steepening OD within 1 month, thus meeting the progression qualifications for epithelial-off corneal crosslinking in both eyes.
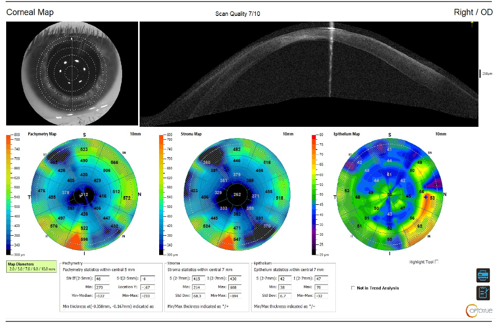
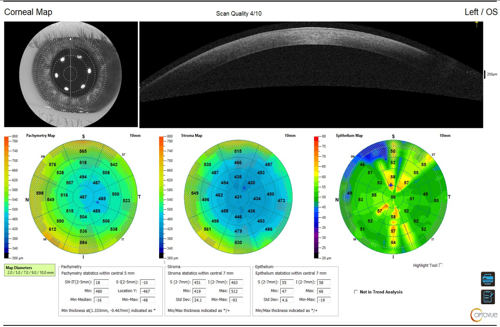
Traditional tomography devices do not allow for the mapping of the corneal epithelium and provide only a total pachymetry value. Due to the extreme thinning in the patient’s right eye, it was vital that the clinician assessed the true stromal thickness on a device capable of epithelial mapping value prior to qualifying the eye for epithelial-off corneal crosslinking. This was done with the Optovue Solix (Visionix) utilizing optical coherence tomography (OCT)/optical coherence tomography-angiography (OCT-A) epithelial mapping (Figures 4 and 5).
Discussion
The advent of corneal crosslinking as a tool in our keratoconus toolbox is one that has changed the prognosis of the condition completely. A condition that once was known to result in a near-definite fate of corneal transplantation is now one that can be managed and slowed to preserve vision.1 As such, it is critical that practitioners screen for and diagnose keratoconus early in the course of the disease and monitor for progression routinely to prevent sight loss in their patients.
Corneal crosslinking is indicated in cases of progressive corneal ectasia. Progression is defined differently by different entities; however, the most widely accepted criteria include steepening of 1 D of any keratometry value, thinning of the thinnest point by 2% to 5%, refractive shift of -0.50 D spherical equivalent, or a reduction in best-corrected visual acuity (BCVA) of 1 line or more.2 These criteria are often time-bound to within 1 year. The patient discussed in this case report definitively meets the progression criteria in both eyes even within 1 month; however, additional aspects of the case, such as corneal thickness, must be considered prior to qualifying the patient for surgery.
Intraoperatively, the surgeon must achieve a post-debridement thickness of 400 µm or greater. This thickness must be confirmed prior to the initiation of ultraviolet irradiation to prevent iatrogenic damage to the endothelium. In cases where the post-debridement thickness is less than 400 µm, hypotonic riboflavin formulations can be used to induce stromal swelling for protection of the corneal endothelium.
One aggregate study found that the average achievable rate of corneal swelling is approximately 10 µm per 30 seconds, with the steepness of the cornea being the largest factor to modulate that rate.3 Steeper corneas are known to swell faster than flatter corneas. Very little data exist on corneas with thicknesses less than 300 µm; thus, the ability to understand the corneal dynamics and potential risks associated with significant amounts of intraoperative corneal swelling is limited.4 For this reason, it is crucial that surgeons managing patients with extreme corneal thinning have an understanding of the epithelial thickness prior to entering the operating room.
Because imaging techniques have improved, it is now understood that one of the early signs of keratoconus includes epithelial remodeling. As the stroma begins to protrude forward, the epithelium will thin over the corneal apex and thicken in a circumferential pattern to maintain the anterior corneal curvature.5 Based on this understanding, we cannot assume that a keratoconic eye has the standard 50-µm epithelium prior to performing an epithelial debridement. In this patient case, the epithelium has remodeled, and the residual stromal bed thickness is a mere 262 µm—significantly less than the minimum-required 400 µm prior to irradiation. The significant epithelial remodeling can be seen in the OCT scan shown in Figure 6.

OCT imaging in conjunction with slit lamp examination of the patient also reveals a lack of corneal clarity, with the inferior scarring on the right cornea. One of the known complications following corneal crosslinking is corneal haze. This haze is rarely visually significant; however, it is one of the most common causes of reduced BCVA following corneal crosslinking.6 It has been found that the best predictor for visually significant corneal haze and scarring following a corneal crosslinking procedure is preoperative densitometry. A clearer preoperative cornea is less likely to develop visually significant haze and scarring than a cornea that is less clear prior to the procedure.7
The value of the ability to image the remodeled corneal epithelium and understand the residual stromal bed thickness prior to surgery cannot be understated in this case. Without that information, an informed decision could not have been made as confidently. Due to the extremely low corneal stroma thickness, along with significant baseline corneal haze and scarring, it was decided after conversation with the patient and his caregivers that performing a crosslinking procedure with epithelial debridement on the right eye was not the best option at this time.
The patient and his parents were informed of the newly FDA-approved epithelium-on procedure that may give more flexibility for thinner corneas, as the epithelium is not completely removed with this approach. It was decided that the patient would proceed with corneal crosslinking on the left eye only, which was completed without complication and maintained the patient’s 20/20 uncorrected VA. A scleral lens fitting is being initiated in the right eye with a scleral lens corrected VA of 20/80. After consultation with a corneal specialist, a corneal transplant is not being pursued at this time due to the patient’s age.
Conclusion
Although the perfect answer for the management of this case is not clear, more knowledge of the corneal condition and more data regarding the epithelial thickness gives the provider and family power to make an informed decision. Postponing corneal crosslinking on an eye with keratoconus that is already severe is certainly not ideal; however, a risk-benefit analysis leans toward waiting for a better alternative and managing vision in the meantime. When the clinical picture does not yield a perfect outcome, increase your testing and data to assist you in your clinical decision-making.
References
- Chunyu T, Xiujun P, Zhengjun F, Xia Z, Feihu Z. Corneal collagen cross-linking in keratoconus: a systematic review and meta-analysis. Sci Rep. 2014;4:5652. doi:10.1038/srep05652.
- Galvis V, Tello A, Ortiz AI, Escaf LC. Patient selection for corneal collagen cross-linking: an updated review. Clin Ophthalmol. 2017;11:657-668. doi:10.2147/OPTH.S101386
- Syed Z, Yu J, Crespo M, Daher ND, Chang CY. Dynamics of corneal swelling with hypoosmolar riboflavin after induction during corneal collagen crosslinking in patients with progressive keratoconus. Cornea. 2024;44(5):567-574. doi:10.1097/ICO.0000000000003609
- Mohammadi F, McGuinness MB, Mustafa MZ, Chong EW, Daniell M. Effectiveness and safety of cross-linking in keratoconus patients with corneal thickness <400 µm: a systematic review and meta-analysis. Am J Ophthalmol. 2026;281:363-383. doi:10.1016/j.ajo.2025.09.039
- Silverman RH, Urs R, Roychoudhury A, Archer TJ, Gobbe M, Reinstein DZ. Epithelial remodeling as basis for machine-based identification of keratoconus. Invest Ophthalmol Vis Sci. 2014;55(3):1580-1587. doi:10.1167/iovs.13-12578
- Dhawan S, Rao K, Natrajan S. Complications of corneal collagen cross-linking. J Ophthalmol. 2011;2011:869015. doi:1155/2011/869015
- Koc M, Uzel MM, Tekin K, Kosekahya P, Ozulken K, Yilmazbas P. Effect of preoperative factors on visual acuity, corneal flattening, and corneal haze after accelerated corneal crosslinking. J Cataract Refract Surg. 2016;42(10):1483-1489. doi:10.1016/j.jcrs.2016.08.017

This content is sponsored by Visionix